Download presentation
Presentation is loading. Please wait.

1
The Heart and Heart Failure in the Year 2013 Jonathan D. Rich, MD Associate Director, Mechanical Circulatory Support Program Bluhm Cardiovascular Institute Assistant Professor of Medicine Northwestern University Feinberg School of Medicine

2
Outline Basics of the heart and the cardiovascular system Define the term “heart disease” Heart disease risk factors and prevention Heart Failure as a major consequence of heart disease Treatment of heart failure in 2013 Q and A

3
Since 1900, heart disease has been the No. 1 killer in the United States every year but 1918 Nearly 2,600 Americans die of heart disease each day, an average of 1 death every 33 seconds Almost 150,000 Americans killed by heart disease each year are under age 65

4
The Heart Basics A muscle about the size of your fist Weighs approximately one pound Is located behind and slightly to the left of the breastbone Pumps about 5 liters of blood every minute

5
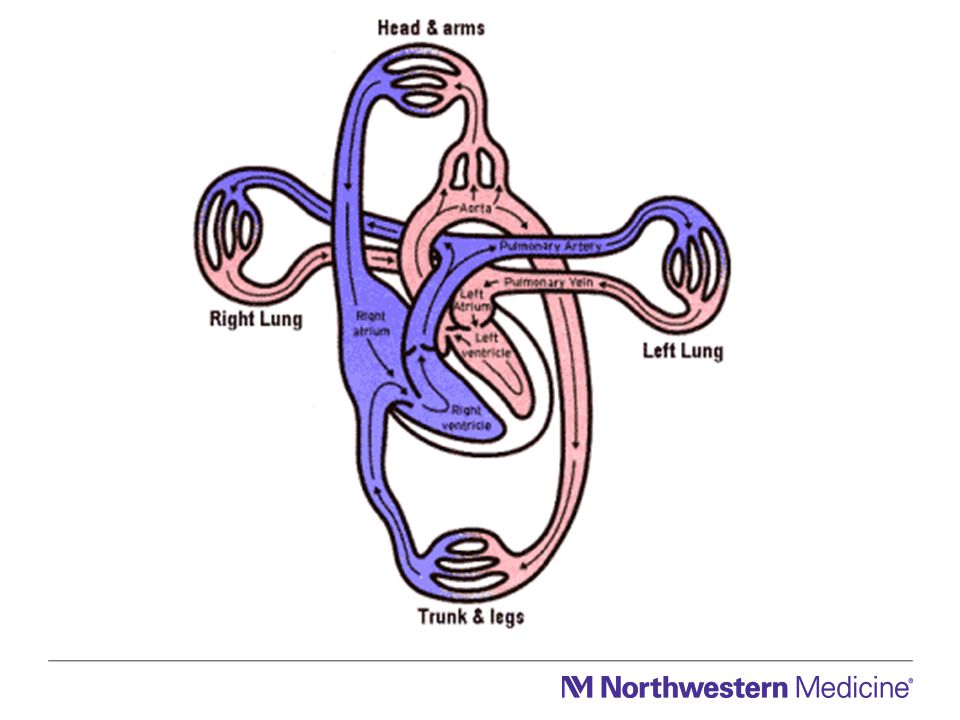
Major Function of the Heart Pump blood through the lungs to refresh the blood with oxygen and remove carbon dioxide The oxygenated blood is pumped to the body to provide oxygen and nutrients and to remove waste products The coronary arteries are the blood vessels that supply blood and oxygen to the heart

7
What exactly is heart disease? Any disease that affects the heart Because coronary artery disease is so common, many people use the term “heart disease” synonymously with “coronary artery disease”

8
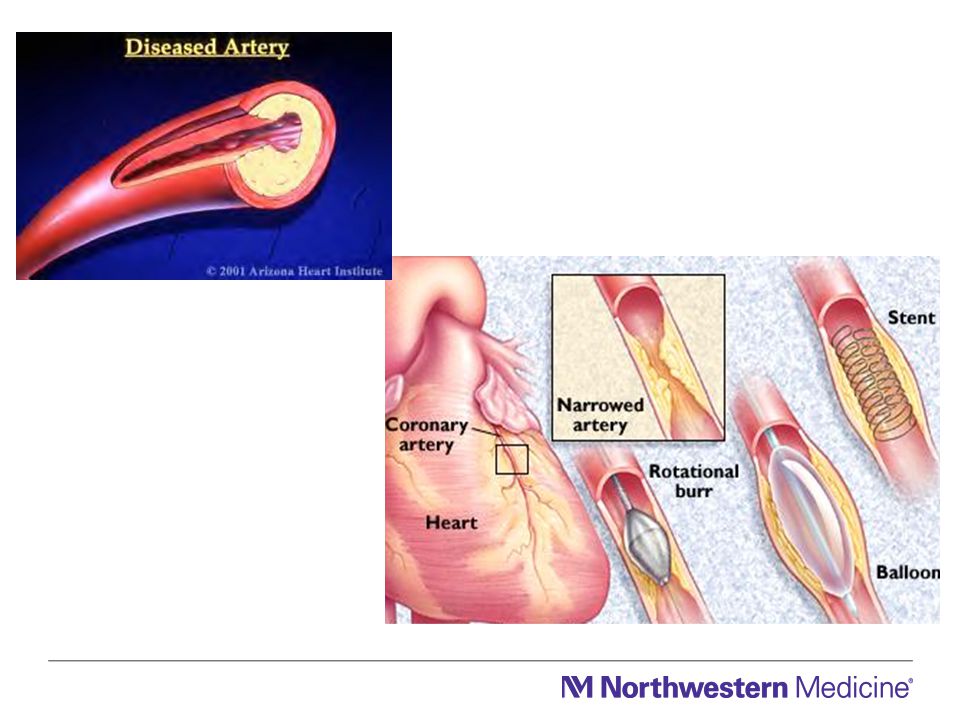
Coronary Artery Disease Coronary artery disease is one of the most common causes of heart disease. Fatty deposits build up in blood vessel walls causing narrowings, called atherosclerosis. Over time, this can lead to a complete blockage of the coronary artery and a “heart attack”.

10
High cholesterol High blood pressure Diabetes Smoking Obesity Lack of physical activity Genetics Heart Disease Risk Factors

11
Uncontrollable Sex Race Age Genetics

12
Heart Disease Risk Factors Uncontrollable Sex Race Age Genetics Controllable High cholesterol High blood pressure Diabetes Smoking Physical activity Obesity Stress and anger

13
Get regular medical checkups. Control your blood pressure. Check your cholesterol. Don’t smoke. Maintain a healthy weight Avoid diabetes Exercise regularly. Manage stress. Choose your parents wisely!

14
Heart Failure: Incidence and Prevalence Approximately 5,000,000 Americans currently suffer from heart failure Approximately 500,000 new cases of heart failure are diagnosed each year Among those with heart failure, approximately 250,000 have “advanced” or Stage D heart failure Nearly 1,000,000 hospital discharges per year for heart failure and the most frequent cause of hospitalization in the elderly Given the burden of heart failure, emphasis on aggressive, guidelines-based medical heart failure therapy is critical. 1 World Health Statistics, World Health Organization, 1995. 2 American Heart Association, 2002 Heart and Stroke Statistical Update.

15
Heart Failure What is Heart Failure? A. The heart is not pumping/squeezing as well as it should (aka systolic heart failure) B. The heart is not relaxing as well as it should (aka diastolic heart failure) Usually, the heart has been weakened by an underlying condition(s) –Blocked coronary arteries/heart attack –High blood pressure –Heart valve abnormalities –Viral infection –Other/unknown
 B. The heart is not relaxing as well as it should (aka diastolic heart failure) Usually, the heart has been weakened by an underlying condition(s) –Blocked coronary arteries/heart attack –High blood pressure –Heart valve abnormalities –Viral infection –Other/unknown.")
16
Heart Failure Heart failure can involve the left or right side of the heart (or both sides) In the majority of cases, the left side is affected first Heart failure occurs when either side of the heart cannot keep up with the demands placed on it to provide sufficient blood flow to the body
 In the majority of cases, the left side is affected first Heart failure occurs when either side of the heart cannot keep up with the demands placed on it to provide sufficient blood flow to the body")
17
Heart Failure How quickly does heart failure develop? It depends –Often a chronic disease with a slow, insidious onset –Other times can develop rapidly (i.e. after a large heart attack or an acute viral infection). The heart tries to compensate for the loss in pumping function by: –Developing more muscle mass –Enlarging itself –Pumping faster
. The heart tries to compensate for the loss in pumping function by: –Developing more muscle mass –Enlarging itself –Pumping faster.")
18
Natural History of HF Survival (%) LV Dysfunction and Symptoms Mechanism of Death Sudden death40% Worsened HF40% Other20% Progression Annual Mortality 0%0% 100% Asymptomatic MildModerateSevere <5% 10%20%–30%30%–80%
 LV Dysfunction and Symptoms Mechanism of Death Sudden death40% Worsened HF40% Other20% Progression Annual Mortality 0%0% 100% Asymptomatic MildModerateSevere <5% 10%20%–30%30%–80%")
19
Yancy CW, Strong M. Prim Care Spec Ed. 2002;6:15 High Risk: Hypertension, coronary artery disease, diabetes, family history of cardiomyopathy Asymptomatic LVD: Previous MI, LV systolic dysfunction, asymptomatic valvular disease Symptomatic HF: Known structural heart disease, shortness of breath and fatigue, reduced exercise tolerance Refractory End-Stage HF: Marked symptoms at rest despite maximal medical therapy A B C D Disease Progression of HF ACC/AHA Stages

20
Heart Failure Treatment Objectives First Objective: Improve survival Second Objective: Improve quality of life – Reduce symptoms – Improve exercise capacity – Reduce hospitalizations – Slow the progression of the disease The more common forms of heart failure often cannot be cured, but they can be effectively treated

21
Yancy CW, Strong M. Prim Care Spec Ed. 2002;6:15 High Risk: Hypertension, coronary artery disease, diabetes, family history of cardiomyopathy Asymptomatic LVD: Previous MI, LV systolic dysfunction, asymptomatic valvular disease Symptomatic HF: Known structural heart disease, shortness of breath and fatigue, reduced exercise tolerance Refractory End-Stage HF: Marked symptoms at rest despite maximal medical therapy A B C D Disease Progression of HF ACC/AHA Stages

22
Yancy CW, Strong M. Prim Care Spec Ed. 2002;6:15 PLUS inotropes, transplant, ventricular assist device Treat hypertension and lipids, smoking cessation, exercise, limit alcohol, ACE inhibitors in appropriate populations PLUS ACE inhibitors, ARB, beta blockers, and aldosterone receptor antagonists in appropriate populations PLUS ACE inhibitors, beta blockers, diuretics, digoxin, aldosterone receptor antagonists, dietary salt restriction Progression of HF Therapy

23
Heart Failure Medications: The Cornerstone of HF Therapy Beta Blockers Ace Inhibitors Aldosterone antagonists Diuretics Digoxin Others

24
Heart Failure Device Therapy -Defibrillator (ICD) -Biventricular Pacemaker -Combined ICD and BIV pacemaker Surgery and/other Procedures –Angioplasty –Coronary artery bypass surgery –Valve replacement Surgical Percutaneous
 -Biventricular Pacemaker -Combined ICD and BIV pacemaker Surgery and/other Procedures –Angioplasty –Coronary artery bypass surgery –Valve replacement Surgical Percutaneous")
26
Heart Failure: Advanced Treatment Options Heart transplantation Left ventricular assist devices (LVAD) A: Bridge to transplantation B: “Destination therapy”
 A: Bridge to transplantation B: Destination therapy")
27
The Right Time for Advanced Heart Failure Therapy “Perfect Window” Operative Risk Clinical severity of heart failure End-organ dysfunction Death Too early Too late

28
HEART TRANSPLANTS Kaplan-Meier Survival (Transplants: January 1982 - June 2010) ISHLT 2012 Survival is based on adult and pediatric transplant recipients N = 96,273 N at risk at 25 years = 112 J Heart Lung Transplant. 2012 Oct; 31(10): 1045-1095
:")
29
NUMBER OF HEART TRANSPLANTS REPORTED BY YEAR ISHLT NOTE: This figure includes only the heart transplants that are reported to the ISHLT Transplant Registry. As such, this should not be construed as evidence that the number of hearts transplanted worldwide has declined in recent years. J Heart Lung Transplant 2008;27: 937-983 2008

31
Heart Transplantation

32
Rise of the Machines INTERMACS

33
First Generation VADs

34
HeartMate Implantable Pneumatic (IP) LVAS HeartMate Vented Electric (VE) LVAS 1995 1997
 LVAS HeartMate Vented Electric (VE) LVAS")
35
Second Generation VADs

36
First Generation Pulsatile LVAD

37
Second Generation Continuous flow LVAD

38
Continuous flow LVADs N Engl J Med 2007;357:885-96

39
Continuous Flow LVADs

40
3 rd Generation Continuous Flow LVADs

41
Next Generation Continuous Flow LVADs

Similar presentations















 failure is the state in which the heart is unable to pump blood.>")

, means your heart can't pump enough blood to meet your body's.>")

>")


